If Obesity Is Universal, Why Does Every Country Treat It Differently?
Biology gives us bodies. Culture decides what they mean.
The most trustworthy source of food and
fitness journalism in the country.
Welcome to Truth Be Told, the weekly food and fitness newsletter published by The Whole Truth Foods.
Editor’s note: Today’s piece from Akshat Kharbanda asks a simple question: if obesity is rising everywhere, why does every country treat it so differently? Drawing from living in five countries and analysing obesity perception at Novo Nordisk’s Denmark headquarters, Akshat maps five radically different cultural scripts about the same biology.
— Samarth Bansal (samarth@thewholetruthfoods.com)
“Beta,” the aunty smiled, spooning biryani onto my plate until it spilled over. An hour later, the same aunty pointed the same spoon across the room “God, she’s gained so much weight!”
I laughed at that contradiction, until I realised it wasn’t hers alone. We’re all walking contradictions when it comes to bodies.
Obesity has doubled globally since 1990. One in eight adults worldwide now lives with obesity. We like to think of it as a universal problem with a scientific solution.
Allow me to raise my spoon.
The biology might be consistent, but what obesity means—morally, socially, economically—changes the moment you cross a border. And meaning determines everything: who gets care and who gets blamed, which bodies are celebrated and which are controlled, whether obesity is a crisis or a goal.
Here’s the thing: Biology gives us the body. Culture gives it meaning. And culture, unlike biology, is something we’ve built, not something we’re born with.
Which means if we want to understand why obesity rates keep rising everywhere despite completely different approaches, we can’t just look at the science. We have to look at the cultural scripts that decide what obesity even means before the first policy is written or the first diet is prescribed.
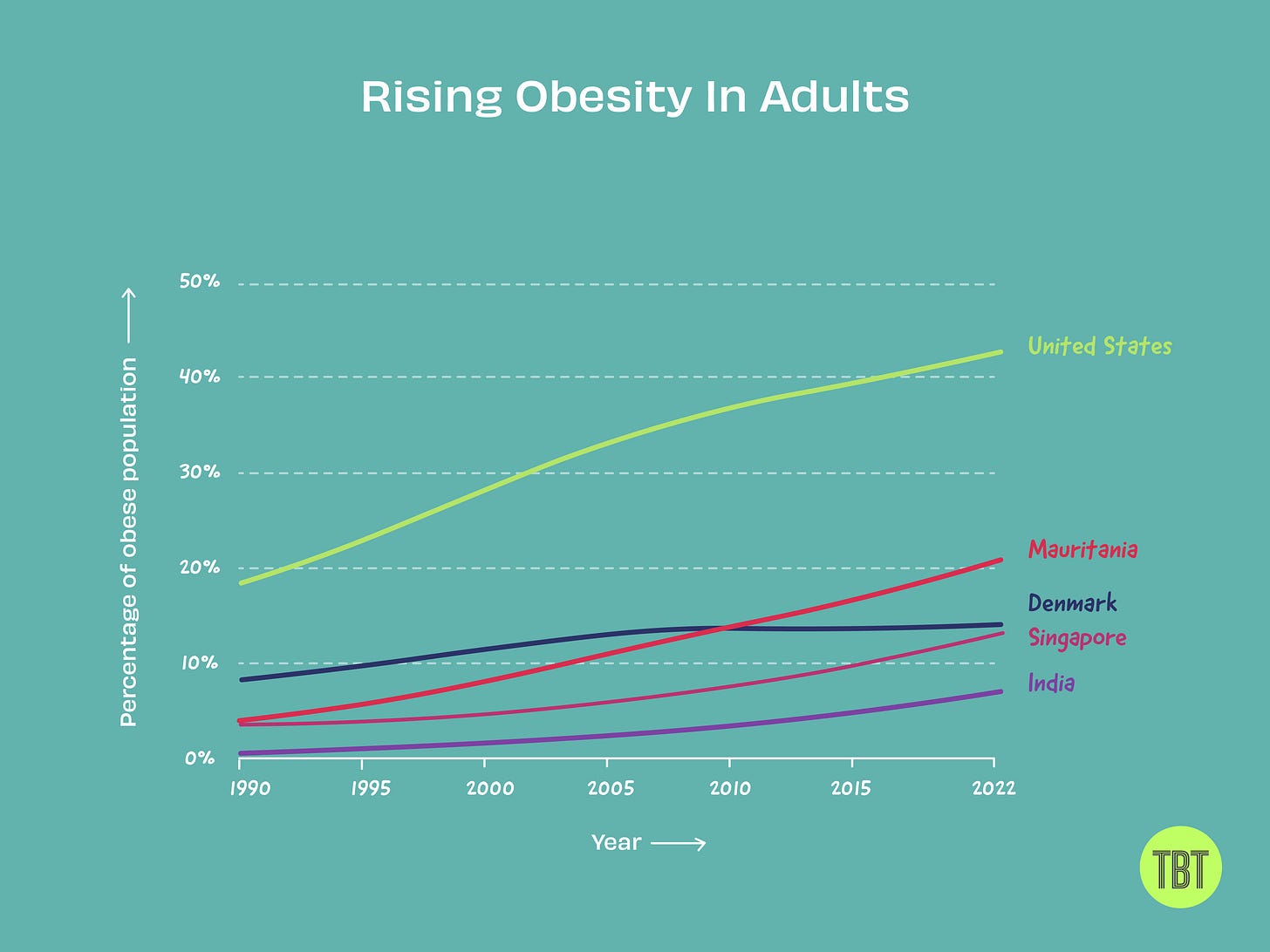 Illustration by Saumya Bansal
Illustration by Saumya BansalThere are 196 countries in the world. Today, we look at five: the United States, Denmark, Singapore, India, and Mauritania, with radically different cultural scripts about the same biology.
But first, we need a map.
Mapping the Contradictions
How do we make sense of a world where the same body means completely different things depending on where you stand?
We need a framework that can hold contradiction without flattening it. Something that lets us see patterns.
I borrowed a method from Erin Meyer’s The Culture Map. Meyer is a business professor who maps how cultures differ on spectrums. It’s meant to help managers navigate cross-cultural teams: why your German colleague gets straight to criticism while your American colleague starts with compliments.
If culture shapes how we work together, it definitely shapes how we see bodies.
So I took her mapping method and applied it to obesity. Instead of plotting communication styles, I mapped how cultures think about obesity across four dimensions. Four questions every culture answers differently:
Dimension 1: Is something wrong? Acceptance ←→ Denial Does the culture acknowledge obesity as an issue or deny it exists/matters?
Dimension 2: Why is it wrong? Health ←→ Aesthetics Is obesity framed as a medical problem or an aesthetic/social one?
Dimension 3: Whose fault is it? Individual ←→ Institutional Does responsibility fall on the person or on systems, policies, and environments?
Dimension 4: How do we fix it? Supportive ←→ Punitive Are interventions compassionate (treatment, access, policy) or punitive (stigma, surveillance, shame)?
Each culture sits somewhere on these four spectrums. Plot them, and you start to see something: there’s no “right” approach. Just different combinations of care and control, each with the stories it tells to justify itself.
Let me show you what I mean.
Five Cultural Scripts
I. United States
Acceptance + Health + Individual + Punitive
In America, everyone knows obesity is a problem. You can walk into any grocery store, any gym, any doctor’s office, and feel the country negotiating its relationship with its own body. The culture has decided this is both a disease (medicalization, GLP-1 boom, “obesity is a chronic condition”) and a moral failure (poor discipline, bad choices, weakness).
That contradiction is everywhere. More than four in ten American adults now live with obesity, according to the CDC. The percentage of US adults experiencing weight-related stigma? Nearly identical.
Oh, and it’s all on you. In all my surveys, the pattern was clear: Americans overwhelmingly believe obesity is the individual’s fault. Personal responsibility. Your choices. Your discipline.
This is the American Dream in action—the story that success comes from hard work and failure from laziness. For that mythology to survive, obesity must stay personal. Because if it’s systemic, if it’s about the environment you’re born into rather than the choices you make, the narrative collapses.
So we ignore the systems. Like the fact that around 60% of supermarket staples in the US are ultra-processed foods, compared to 15% in Europe. Or that American portion sizes dwarf those elsewhere—a McDonald’s large drink is 89% bigger in the US than in the UK.
These aren’t personal failures. They’re designed environments. But acknowledging that threatens the dream. So the story stays: your body, your fault.
Entire industries depend on this contradiction. The diet industry, the wellness industry, the pharmaceutical industry—all profit from treating obesity as both a disease and a personal failure. Cure it completely, or remove the stigma entirely, and the business model breaks.
The paradox is the product.
II. Denmark
Acceptance + Health + Institutional + Supportive
Walk into a Danish health clinic and you won’t hear lectures about willpower or discipline. Obesity is viewed as a public health issue shaped by environments, policies, and infrastructure. And that is society’s responsibility to fix, not just yours.
The approach is supportive. No one’s shouting “no excuses” here. Everyone’s cycling to work, eating rye bread, and talking about balance. On paper, this sounds enlightened.
And yet.
Obesity in Denmark has tripled since 1987, from 6.1% to 18.4% by 2021. Despite all that systemic thinking and supportive infrastructure, rates keep climbing.
Here’s where the logic breaks: If obesity is society’s problem, society should act. In 2011, the government tried. They introduced a “fat tax” on foods high in saturated fat—a real policy intervention to shift behaviour at scale.
Within a year, the fat tax was gone. Public backlash was instant. Politicians feared losing elections. Consumers crossed borders for cheaper butter. The one policy that could have actually changed behaviour was rejected by culture.
Because it turns out Denmark values something more than preventing obesity: Livskvalitet—life quality. The culture that cycles everywhere also serves cake at every meeting. Balance is the ideal, and balance means nobody gets to tell you what to eat.
So while Denmark frames obesity as society’s responsibility, solving it would require society to give something up. And Denmark has shown signs that it won’t.
The paradox is the choice.
III. Singapore
Acceptance + Aesthetics + Individual + Punitive
Singapore acknowledges obesity openly. But the concern isn’t really health. It’s aesthetics. K-pop beauty standards, Instagram influencers, cosmetic surgery ads… and it starts early.
In a nation built on optimisation, the body is just another KPI to perfect.
That instinct gave rise to the (in)famous Trim and Fit program, launched in 1992 to make students “fit for the nation.”
The idea was to identify overweight kids, put them through extra workouts, and monitor their diets. But this led to humiliation: public weigh-ins became rituals of shame and playground teasing was enabled by policy.
By 2007, after years of criticism for promoting stigma and eating disorders, the program was scrapped.
But its logic never left. The state may have softened its tone, but society didn’t. The expectation remains: your body reflects your discipline.
And yet, obesity keeps rising. Using Asian BMI cutoffs—which account for higher health risks at lower weights—58% of Singaporean adults now have an unhealthy weight. Youth obesity has climbed even as the aesthetic bar rises higher.
Optimise harder, get worse results.
The paradox is the optimisation.
IV. India
Denial + Aesthetics + Individual + Punitive
India has the highest share of underweight adults globally. India is also the third most obese country in the world.
Both things are true. Welcome to the double burden of malnutrition.
On one side: rapid urbanisation, sedentary lifestyles, and the flood of processed foods into cities have driven obesity rates up. On the other: India still has the world’s largest population of undernourished people.
Different populations, same country. One eating too little, the other eating too much of the wrong things.
Here’s the paradox: Public health policy still fights the old war. Malnutrition gets national programs, subsidised grains, policy attention. But obesity… that’s your problem. An individual failure, not a public health crisis.
And when obesity gets acknowledged, it becomes a matter of aesthetics, marriage markets, and social acceptability. According to a 2023 obesity survey, 70% of respondents said people face bullying or teasing due to their weight in workplaces and social settings.
 Illustration by Sayali Kulkarni and Alfred Anthony
Illustration by Sayali Kulkarni and Alfred AnthonyThe state subsidises staples to fight undernutrition. Private markets flood the same cities with cheap processed foods. India chases one crisis while creating the other.
The paradox is the duality.
V. Mauritania
Denial + Aesthetics + Institutional + Supportive
In Mauritania, the story flips completely. Here, obesity isn’t a problem to be fixed but a beauty to be maintained. Larger bodies symbolize wealth, fertility, and marriageability. Abundance signals success.
A bigger body means a better marriage, and therefore, security. In a world where marriage defines survival, parents fatten their daughters out of love.
That belief takes physical form in a practice called leblouh. Girls, some as young as six, are made to consume up to 14,000-16,000 calories a day—almost four times what an adult male bodybuilder eats.
Refusal isn’t an option. In some cases, toes are crushed between sticks or skin pinched to force them to eat.
Mauritania has one of the highest female obesity rates in Africa while male obesity sits among the lowest quartile in the world.
Entire families participate. Communities celebrate it. The government doesn’t intervene—why would it? Culturally, there’s nothing wrong. Obesity here is institutional, supportive, desired.
And yet the health consequences are identical to countries fighting obesity. Same disease, opposite meaning. The same act that causes harm is called care.
How do you solve a problem that isn’t seen as a problem? You can’t. A culture so committed to protecting its daughters ends up harming them instead.
The paradox is the care
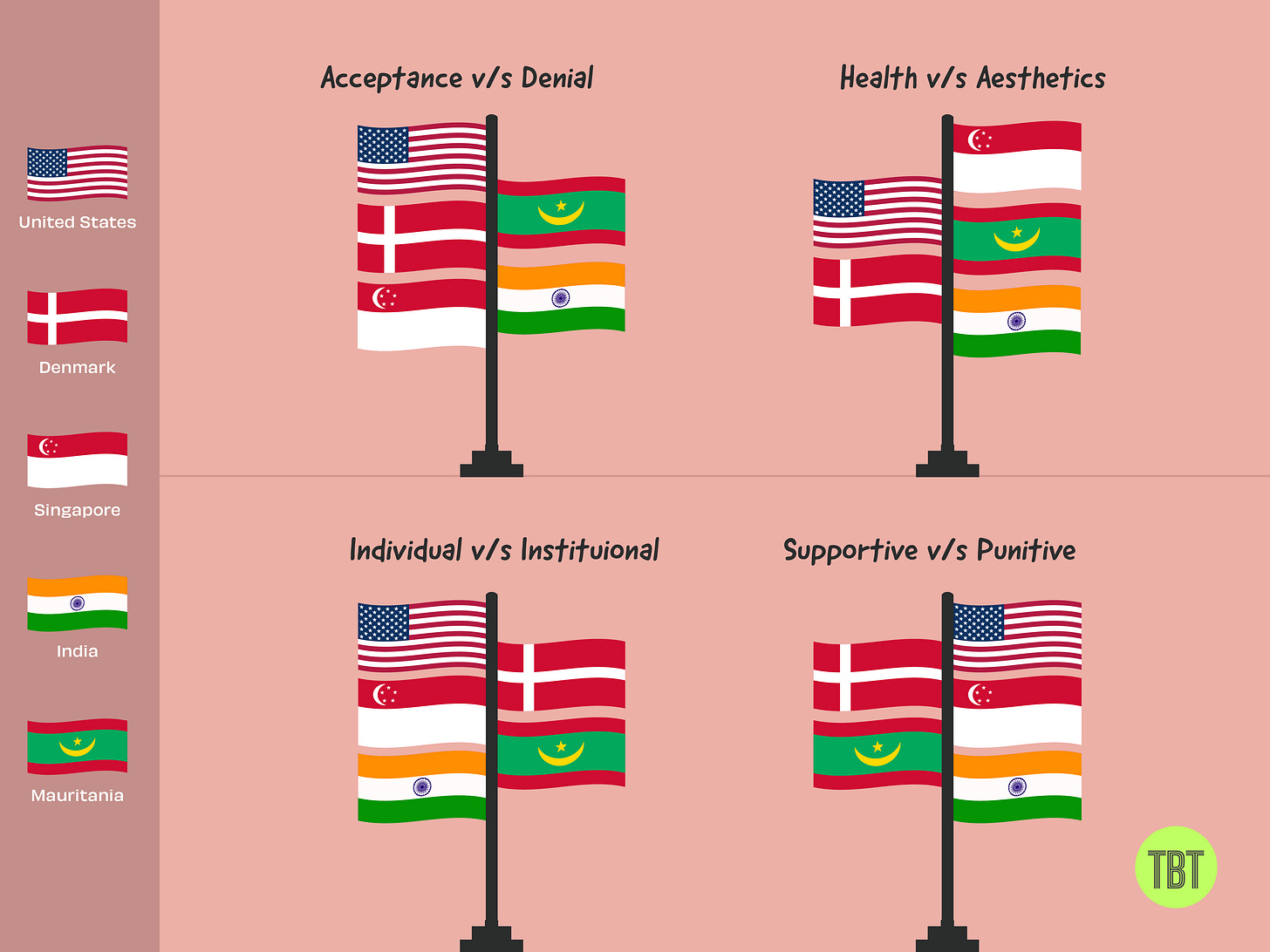 Illustration by Saumya Bansal.
Illustration by Saumya Bansal.Why This Matters
So what? Why does any of this matter beyond cultural trivia?
Because how we define a body decides how we treat it.
Obesity may begin in biology, but it unfolds in culture. And culture decides everything that follows: who gets care and who gets blamed, which bodies are celebrated and which are controlled, whether the problem is you or the world you live in.
Science may diagnose disease, but culture decides which ones deserve care.
Right now, obesity rises everywhere—across all five countries, across all approaches. The meanings just distribute the suffering differently. America profits from it. Denmark preserves comfort despite it. Singapore optimises around it. India denies half of it. Mauritania celebrates it.
None of these stories are really about obesity. They’re about what each culture refuses to give up.
Look, every culture thinks its approach makes sense. None do.
But here’s the thing: if meaning is cultural, it isn’t fixed. It shifts with time, with voices, with who gets heard. And if meaning is cultural, it’s also ours to redefine.
Maybe that’s where the real work begins. Not in finding the right policy or the right program, but in changing the stories we tell about bodies.
Because right now, every culture’s story serves its values first and its people second.
Here is a short feedback form to help us understand how we’re doing. Would you please share your thoughts? Link here. Thank you!








